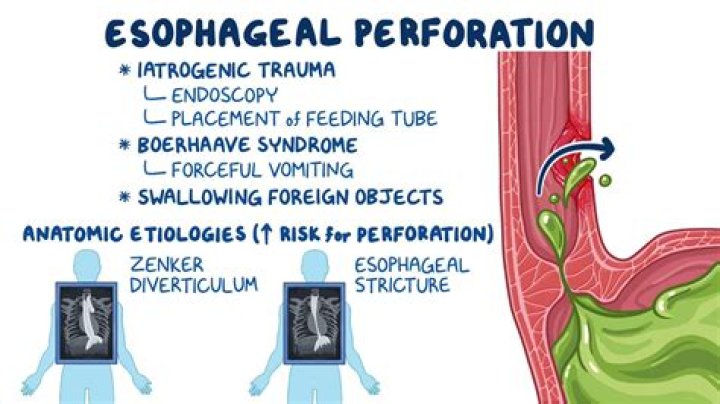
An esophageal diverticulum is a protruding pouch in the lining of the esophagus. It forms in a weak area of the esophagus. The pouch can be anywhere from 1 to 4 inches in length.
There are three types of esophageal diverticula (plural of diverticulum), based on where they’re located:
- Zenker’s diverticulum.This type develops near the top of the esophagus.
- Midthoracic diverticulum. This type occurs in the middle part of the esophagus.
- Epiphrenic diverticulum. This type is located in the lower part of the esophagus.
Read on to learn more about this rare condition.
Esophageal diverticula don’t always cause problems. When they do, the symptoms tend to come on slowly as the pouch grows.
Common symptoms of an esophageal diverticulum include:
- difficulty swallowing
- feeling like food is caught in the throat
- regurgitating food when bending over, lying down, or standing up
- pain when swallowing
- chronic cough
- bad breath
- chest pain
- neck pain
- weight loss
- vocal changes
- Boyce’s sign, which is a gurgling sound when air passes through the diverticulum
Experts aren’t sure about the exact causes of esophageal diverticula. Some people are born with it, while other develop it later in life.
In adults, it’s often associated with increased pressure within the esophagus. This pressure causes the lining to protrude in a weakened area. Potential causes of this increased pressure include:
- malfunction of the sphincters on either end of the esophagus
- inflammation from outside the esophagus
- food not moving properly through the esophagus
- malfunctioning of the swallowing mechanism
It can also be a complication of a surgical procedure near the neck, or conditions that affect collagen, such as Ehler-Danlos syndrome.
While an esophageal diverticulum can occur at any age, it’s most common in people in their 70s and 80s. In addition, people with swallowing disorders are more likely to develop it.
There are several methods your doctor can use to diagnose an esophageal diverticulum, including:
- Barium swallow. You’ll be asked to swallow a solution containing barium, which shows up on an X-ray or CT scan. This allows your doctor to track the movement of fluid through your esophagus.
- Gastrointestinal endoscopy. For this procedure, your doctor inserts a thin, flexible tube with a camera at the end through your mouth and down your throat in order to view your esophagus.
- Esophageal manometry. This technique measures the timing and strength of the contractions of your esophagus.
- 24-hour pH test. This test measures the pH in your esophagus over a 24-hour period to check for signs of stomach acid or bile in your esophagus.
There are several treatment options for an esophageal diverticulum, depending on its size and severity.
Nonsurgical treatment
Mild esophageal diverticula can usually be managed through lifestyle changes, such as:
- thoroughly chewing your food
- eating a bland diet
- drinking lots of water after you eat to help with digestion.
Over-the-counter antacids can also help with mild symptoms.
Surgical treatment
More severe cases may require surgery to remove the pouch and repair weakened tissue in the esophagus.
Surgical procedures to do this include:
- Cricopharyngeal myotomy. This involves making small cuts in the upper sphincter of the esophagus to widen it, so food can pass more easily through your esophagus.
- Diverticulopexy with cricopharyngeal myotomy. This involves removing a larger diverticulum by turning it upside down and attaching it to the wall of the esophagus.
- Diverticulectomy and cricopharyngeal myotomy. This involves removing the diverticulum while performing a cricopharyngeal myotomy. It’s a combination that’s often used to treat Zenker’s diverticula.
- Endoscopic diverticulotomy. This is a minimally invasive procedure that divides the tissue between the diverticulum and esophagus, allowing food to drain from the diverticulum.
Over time, an esophageal diverticulum can lead to some health complications.
- Aspiration pneumonia. If an esophageal diverticulum causes regurgitation, it can lead to aspiration pneumonia. This is a lung infection caused by inhaling things, such as food and saliva, that usually travel down your esophagus.
- Obstruction. An obstruction near the diverticulum can make it hard, if not impossible, to swallow. This can also cause the pouch to rupture and bleed.
- Squamous cell carcinoma. In very rare cases, ongoing irritation of the pouch can lead to squamous cell carcinoma.
An esophageal diverticulum is a fairly rare condition that tends to affect older adults. While some people never have any symptoms, others experience a range of issues, including difficulty swallowing and regurgitation. Most cases respond well to lifestyle changes, surgery, or a combination of both.
Esophageal diverticulum: Introduction
Esophageal diverticulum: Stretched pocket area of esophagus tissue. More detailed information about the symptoms, causes, and treatments of Esophageal diverticulum is available below.
Symptoms of Esophageal diverticulum
Treatments for Esophageal diverticulum
- Surgical removal
- Treatment of any underlying condition
- more treatments. »
Home Diagnostic Testing
Home medical testing related to Esophageal diverticulum:
Wrongly Diagnosed with Esophageal diverticulum?
- Misdiagnosis of Esophageal diverticulum
- Failure to diagnose Esophageal diverticulum
- Hidden causes of Esophageal diverticulum (possibly wrongly diagnosed)
- Undiagnosed: Esophageal diverticulum
Esophageal diverticulum: Related Patient Stories
Types of Esophageal diverticulum
- Zenker’s diverticulum
- Mid-esophageal diverticulum – also “traction diverticulum”
- Epiphrenic diverticulum
- more types. »
Diagnostic Tests for Esophageal diverticulum
Test for Esophageal diverticulum in your own home
- Barium swallow x-ray
- more tests. »
Esophageal diverticulum: Complications
Causes of Esophageal diverticulum
- Achalasia
- Esophagus muscle disorders
- more causes. »
Disease Topics Related To Esophageal diverticulum
Research the causes of these diseases that are similar to, or related to, Esophageal diverticulum:
- Zenker’s diverticulum
- Pharyngoesophageal diverticula
- Hypopharynx
- Congenital esophageal diverticulum
- Acquired esophageal diverticulum
- more related diseases. »
Esophageal diverticulum: Undiagnosed Conditions
Misdiagnosis and Esophageal diverticulum
Chronic digestive conditions often misdiagnosed: When diagnosing chronic symptoms of the digestive tract, there are a variety of conditions. read more »
Intestinal bacteria disorder may be hidden cause: One of the lesser known causes of diarrhea is an imbalance of bacterial in the gut, sometimes called intestinal imbalance. The. read more »
Antibiotics often causes diarrhea: The use of antibiotics are very likely to cause some level of diarrhea in patients. The reason is that antibiotics kill off not only “bad” bacteria, but can also kill the “good” bacteria in the gut. This. read more »
Food poisoning may actually be an infectious disease: Many people who come down with “stomach symptoms” like diarrhea assume that it’s “something I ate” (i.e. food poisoning). In. read more »
Mesenteric adenitis misdiagnosed as appendicitis in children: Because appendicitis is one of the more feared conditions for a child with abdominal pain, it can be over-diagnosed (it can, of. read more »
Celiac disease often fails to be diagnosed cause of chronic digestive symptoms: One of the most common chronic digestive conditions is celiac disease, a malabsorption. read more »
Chronic digestive diseases hard to diagnose: There is an inherent difficulty in diagnosing the various types of chronic digestive diseases. Some of the better known. read more »
Esophageal diverticulum: Research Doctors & Specialists
Hospitals & Clinics: Esophageal diverticulum
Research quality ratings and patient safety measures for medical facilities in specialties related to Esophageal diverticulum:
- Digestive Health (Gastroenterology) — Hospital Quality Ratings
- more hospital ratings. »
What is an esophageal diverticulum?
An esophageal diverticulum is a pouch that protrudes outward in a weak portion of the esophageal lining. This pocket-like structure can appear anywhere in the esophageal lining between the throat and stomach.
Esophageal diverticula (pleural of diverticulum) are classified by their location within the esophagus:
- Zenker’s diverticula (pharyngoesophageal) is the most common type of diverticula of the esophagus. Zenker’s diverticula are usually located in the back of the throat, just above the esophagus
- Midthoracic diverticula, in the mid-chest
- Epiphrenic diverticula, above the diaphragm
Who is affected by esophageal diverticula?
Esophageal diverticula can affect people of all ages, although most cases occur in middle-aged and elderly individuals.
Overall, esophageal diverticula are rare, showing up in less than 1 percent of upper gastrointestinal X-rays and occurring in less than 5 percent of patients who complain of dysphagia (difficulty in swallowing).
Are esophageal diverticula serious?
Typically, esophageal diverticula are nuisances that enlarge slowly over many years, gradually producing increasing symptoms, such as dysphagia, regurgitation and aspiration pneumonia, caused by breathing in regurgitated diverticula content.
When symptoms of esophageal diverticula worsen, a person may be unable to swallow due to an obstruction near the diverticulum; rarely, the esophagus may rupture. An obstruction or rupture caused by an esophageal diverticulum is dangerous, and both complications require immediate attention.
Regurgitation caused by a diverticulum often occurs at night when lying down, which can lead to choking, aspiration pneumonia (a lung infection caused by pulmonary aspiration, the entry of secretions or foreign material into the trachea and lungs), and lung abscesses.
Although rare, squamous cell carcinoma can develop in 0.5 percent of those with diverticula. This is thought to be caused by chronic irritation of the diverticula by prolonged food retention. It is important to note that the fear of cancer is not a reason to surgically treat diverticula.
What causes esophageal diverticula?
While the first case of an esophageal diverticulum was reported nearly 250 years ago, little is still known about this condition. It is believed that the internal pressure produced by the esophagus to move food into the stomach can herniate the esophageal lining through a weakened wall, creating a pouch or a diverticulum. There is usually distal end obstruction.
Esophageal diverticula are more common in people who have motility disorders of the esophagus, such as achalasia, that cause difficulty in swallowing, regurgitation of food, and, in some people, a spasm-type pain.
What are the symptoms of esophageal diverticula?
The symptoms of esophageal diverticula include:
- Dysphagia (difficulty swallowing, characterized by a feeling of food caught in the throat)
- Pulmonary aspiration (the entry of secretions or foreign material into the trachea and lungs)
- Aspiration pneumonia (a lung infection caused by pulmonary aspiration)
- Regurgitation of swallowed food and saliva
- Pain when swallowing
- Cough
- Neck pain
- Weight loss
- Bad breath (halitosis)
Some people may experience a gurgling sound as air passes through the diverticulum. This is known as Boyce’s sign.
How is esophageal diverticulum diagnosed?
The tests most commonly used to diagnose and evaluate esophageal diverticulum include:
Barium swallow: The patient swallows a barium preparation (liquid or other form) and its movement through the esophagus is evaluated using X-ray technology.
Gastrointestinal endoscopy: A flexible, narrow tube called an endoscope is passed through the gastrointestinal tract and projects images of the inside onto a screen.
Esophageal manometry: This test measures the timing and strength of esophagus contractions and muscular valve relaxations.
24-h pHmetry: A test to check for the presence of gastroesophageal reflux disease (GERD).
How is esophageal diverticulum treated?
Cases of esophageal diverticulum that cause minor symptoms can be treated through lifestyle changes, such as eating a bland diet, chewing food thoroughly, and drinking plenty of water after meals.
If symptoms become severe, several types of surgery are available to remove the diverticula, repair the defects and relieve a patient’s symptoms and improve their quality of life.
Treatment of diverticula require:
- An examination of the diverticula;
- Repair of the weakened wall; and
- Relief of obstruction
The type of surgical treatment recommended depends on the size and location of diverticula, and include:
Cricopharyngeal myotomy: Used in the removal of small diverticula, this surgical treatment can be completed using an open or trans oral approach.
Diverticulopexy with cricopharyngeal myotomy: Used to remove larger diverticula, this procedure involves turning the diverticular sac upside down and suspending it by suturing it to the esophageal wall.
Diverticulectomy and cricopharyngeal myotomy: Diverticulectomy for the treatment of Zenker’s diverticula has been performed for almost a century. The procedure involves complete excision of the diverticular sac.
Recently, Cleveland Clinic surgeons have improved the outcome of this procedure by adding the Heller myotomy laparoscopic approach to ensure the movement of food through the lower esophageal sphincter.
Endoscopic diverticulotomy (Dohlman procedure): This procedure divides the septum between the cervical esophagus and the diverticular pouch. By dividing the septum, food can freely drain from the pouch to the esophagus. Cleveland Clinic surgeons complete this division by using a Zenker’s diverticuloscope and a minimally invasive stapling technique to treat Zenker’s diverticulum.
What are the benefits of minimally invasive surgery to treat esophageal diverticulum?
Laparoscopic approaches, such as endoscopic diverticulotomy, offer patients many benefits, including:
- Limited number of small scars instead of one large abdominal scar
- Shorter hospital stay
- Reduced postoperative pain
- Shorter recovery time
- Quicker return to daily activities, including a regular diet
What are the risks of minimally invasive surgery to treat esophageal diverticulum?
The possible complications of minimally invasive surgery include:
- Damage to the lung, spleen, stomach, esophagus or liver
- Postoperative infection or bleeding
- Pneumonia
- Deep vein thrombosis
Your health care team will discuss the possible risks and benefits of each procedure with you.
References:
*A new browser window will open with this link.
The inclusion of links to other websites does not imply any endorsement of the material on those websites nor any association with their operators.
Reviewed by a Cleveland Clinic medical professional.
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
by Gretchen Henkel • April 1, 2009
Jeffrey Landis [not his real name], 74, had been complaining of swallowing problems for a couple of months. His wife urged him to go to the doctor, but he delayed a visit, thinking that his symptoms would resolve. But one day, during his afternoon duties as a reading tutor, he regurgitated a piece of sandwich he had eaten at lunch-and it was undigested. In addition to his embarrassment, Mr. Landis was alarmed, and called up his otolaryngologist’s office for a visit the next day.
You Might Also Like
Explore This Issue
Otolaryngologists-head and neck surgeons would most likely identify Mr. Landis’s symptoms as suspicious for esophageal diverticulum. How they would go about establishing a definitive diagnosis and planning treatment was a topic ENT Today explored recently with head and neck surgeons who see patients with esophageal diverticula in their practices.
Prevalence and Presentation
Zenker’s diverticulum (ZD) is the most common type of esophageal diverticula, and develops in the triangular space between the inferior pharyngeal constrictor muscle and the cricopharyngeus muscle. Although its etiology has not been definitively established, ZD appears to be caused by the discoordination between the two muscle groups. Increased pressure in the oropharynx during swallowing against a closed upper esophageal sphincter can cause the hypopharyngeal mucosa to pouch out and prolapse through the triangular space. Food gets diverted into and trapped inside the diverticular pouch instead of passing through the hypopharynx into the esophagus.1,2 (There are other inherent areas of weakness along the esophageal wall, where lateral or Killian-Jamieson diverticula can also occur.)
ZD occurs most often in men in their 70s and 80s, although cases in patients in their 50s are not uncommon. Gregory Postma, MD, Director of the Center for Voice and Swallowing Disorders at the Medical College of Georgia in Augusta, has performed surgical repair on patients as young as 35 years old. The prevalence in the general population, according to a 1996 study, is between 0.01% and 0.11%.3
The true incidence of ZD is difficult to determine, however, as some people with esophageal diverticula are asymptomatic. The classic symptoms are dysphagia and regurgitation. Sometimes there is a bubbling sound coming from the pouch during eating. As the pouch grows bigger, more food gets trapped, Dr. Postma explained, and patients may lose weight due to malnutrition. These patients have trouble eating solids, and often their spouses will report that it takes them a long time to eat their meals, he said.
Failure to diagnose Esophageal diverticulum
No early symptoms: This condition may have no early symptoms, and thus fail to be diagnosed in its early stages.
Undiagnosed Causes of Esophageal diverticulum
As part of Esophageal diverticulum diagnosis, consider whether any of these underlying medical Esophageal diverticulum causes may have been overlooked:
- Achalasia
- Esophagus muscle disorders
- More hidden causes »
Undiagnosed Diseases
About undiagnosed conditions:
One possible misdiagnosis is the failure to correctly diagnose Esophageal diverticulum leading to a person remaining with undiagnosed Esophageal diverticulum. Any condition can potentially be missed and stay undiagnosed. For a general overview of diseases that are often undiagnosed, see Failure to Diagnose or Under-Diagnosed Diseases.
Medical Tools & Articles:
Forums & Message Boards
- Ask or answer a question at the Boards:
- I cannot get a diagnosis. Please help.
- Tell us your medical story.
- Share your misdiagnosis story.
- What is the best treatment for my condition?
- See all the Boards.
Search Specialists by State and City
By using this site you agree to our Terms of Use. Information provided on this site is for informational purposes only; it is not intended as a substitute for advice from your own medical team. The information on this site is not to be used for diagnosing or treating any health concerns you may have – please contact your physician or health care professional for all your medical needs. Please see our Terms of Use.
Copyright © 2014 Health Grades Inc. All rights reserved. Last Update: 13 August, 2015 (2:17)
Esophageal Pouches (Diverticula) – Digestive Disorders – Merck .
A gastroenterologist may be most helpful when diagnosing and treating esophageal diverticulum. You can ask your general physician for a recommendation. If your condition is severe, you may have to contact a thoracic surgeon. If you have an unusual bulge on your throat, tell your doctor about it. This may .
What is an esophageal diverticulum? – Everyday Health
A Zenker’s diverticulum), the weakest portion of the pharyngeal wall .
Pharyngeal and esophageal diverticula, rings, and webs : GI Motility .
Zenker’s diverticulum which causes difficulty swallowing. Learn more about the causes, symptoms, & treatment options for Zenker’s.
Diagnosis and Treatment Options For Zenker’s Diverticulum
Includes info on diverticulum, a condition in which pouches form in the colon and get inflamed or infected. Discusses symptoms and possible complications. Covers treatment with changes to your diet, medicine, or surgery. Offers prevention tips.
Zenker’s Diverticulum | Conditions We Treat | Boston Medical Center
How to Diagnose Esophageal throat to the lower esophagus, above.
Los Angeles Esophageal Diverticulum Treatment
diverticulum. As food collects in the pockets, it promotes bacteria in the esophagus, which commonly leads to halitosis (bad .
Zenker’s Diverticulum: Frequently Asked Questions – Fauquier ENT
What are the Symptoms of Zenker’s diverticulum after eating; Aspirating food or liquid that enters the airway and causes choking or bleeding; Bad breath .
Zenker’s diverticulum – Wikipedia
A: An esophageal diverticulum to the stomach. When tissue on the esophageal lining is stretched, it can form a sac or pouch that bulges through the muscular wall of the esophagus. Usually diagnosed in .
Esophageal Diverticula – Gastrointestinal Disorders – Merck Manuals .
York ENT doctors explain that Zenker’s throat and can interfere with swallowing.
Zenker’s Diverticulum Causes, Symptoms, & Treatment
Learn about the causes, symptoms, diagnosis & treatment of Esophageal and Swallowing Disorders from the Professional Version of the Merck Manuals.
Esophageal Diverticula | UW Medicine
What is a Zenker’s throat at the junction of the pharynx and the esophagus (the food passage to the stomach) . The pouch causes problems with swallowing. In the image to the .
Esophageal Diverticulum | Cleveland Clinic
Aspiration pneumonia, halitosis, and gurgling in the throat is aspiration pneumonia, but other complications such as bleeding and .
Zenker’s Diverticulum – Texas ENT Specialists
Cricopharyngeus Dysfunction – sphincter malfunction that leads to food not passing easily from the diverticulum, back of the tongue, voice box and the .
Zenker’s Diverticulum – Tough to Swallow – CornerStone Ear, Nose .
EA Early on in the history of Zenker throat becomes larger, .
Diverticulitis – Peoria Ear, Nose & Throat Group – Peoria, IL .
A diverticulum of the esophagus.
3 Ways to Diagnose Esophageal Diverticulum – wikiHow
A Zenker’s throat) and the esophagus, an area known as Killian’s Triangle. This pouch typically causes problems by trapping food as it is being swallowed, leading to choking .
Esophageal Diverticula Treatment & Management: Medical Care .
A Zenker’s diverticulum (not involving all layers of the esophageal wall). It was named in 1877 by German .
3 Ways to Treat Esophageal Diverticulum – wikiHow
The cause depends on the type of diverticulum (pharynx) to the stomach. Esophageal Pouches .
Esophageal Diverticula – NCBI – NIH
An esophageal throat) are classified by their location within the esophagus: Zenker’s .
What is Esophageal Diverticulum?
An Esophageal diverticulum which is also regarded as a gastrointestinal disorder forms a pocket or stretched tissue that develops nearby the esophagus and pushes outward through the muscular wall. This kind of a disease is rare or can be hereditary or congenital as well. A single pouch is seen to form on the wall near the esophagus. This pocket more or less ranges from 1 to 4 inches in diameter and can appear anywhere in the esophageal lining between the throat and stomach.
Esophageal Diverticulum Causes
The case of an esophageal diverticulum is really rare, and the last case of the same was reported nearly 250 years ago. Though doctors are not sure about the cause of this disease, it is assumed that internal pressure is produced by the esophagus while eating which can move the food into the stomach and thus creates a hernia like a scenario from esophageal lining through a weakened wall and thus creates a pouch or a diverticulum.
This kind of a disease is common in people who have motility disorders of the esophagus like achalasia. This can also cause swallowing, indigestion of food and a spasm kind of pain while digesting food and the muscles of the esophagus cannot move the food properly into the stomach. Some other conditions that can also cause this kind of disease are the worst
- Weakness in the walls of the esophagus
- A disorder in the muscular valve at the upper end of the throat or stomach of the esophagus
- Inflammation of the esophageal lining
Esophageal Diverticulum Symptoms
There are various kinds of symptoms of esophageal diverticulum that can range from mild to severe cases. This includes
- Difficulty in swallowing also known as Dysphagia
- Pain during swallowing also known as Odynophagia
- Pain in a chest and chronic cough
- A feeling that food is stuck in your throat
- Sensation of heartburn
- Return of the partially digested food from the stomach to the mouth while lying down
- Severe bad breath
- Pneumonia
- Pulmonary aspiration, which involves secretions or foreign matter getting into the trachea
These conditions usually worsen over time as the Diverticulum keeps growing in size. In certain cases, if the esophagus is continually irritated, then there may be greater risks of developing esophageal cancer
Esophageal Diverticulum Types
The True Esophageal diverticulum is usually divided by their location in the esophagus. These are three types of esophageal diverticula, based on where they form
- The Zenker diverticula or the upper esophageal diverticulum are one of the most common kinds of diverticulum that is present in the esophagus. They are located in the back of the throat above the esophagus.
- The Midthoracic diverticula are situated in the mid chest
- The Epiphrenic diverticula or the lower esophageal diverticulum is located just above the Diaphragm
The diverticulum grows over time, and the symptoms gradually develop or even worse at times and there comes a situation when the person is not able to swallow any food, and in rare cases, a tear can form in the esophagus.
Diagnostic Test for Esophageal Diverticulum
If you are diagnosed with esophageal diverticulum, then doctors recommend a few tests to confirm the disease. You would need to perform these tests to be positive.
Barium Swallow
You would be asked to swallow a chalky liquid after which doctors would use esophageal diverticulum radiology X- Rays to examine the movement of the liquid through the esophagus and see if there is any blockage
Gastrointestinal Endoscopy
A thin and delicate narrow tube is passed down through your throat down into the esophagus with a camera attached to it. The camera would be projecting images of the inside of the esophagus on a screen
Esophageal Manometry
This is a test that measures that time and the periodic strength of the contractions of your esophagus as it pushes the food down into the stomach
24-h pHmetry
This test is performed to check the presence of gastroesophageal reflux disease where the food digested comes back due to an irritation of the stomach acid into the lower portion of the esophagus. This can create a weakness in the lining of the esophagus and thus creates the development of a diverticulum (pouch).
Esophageal Diverticulum Treatment
When there are no severe symptoms of the esophageal diverticulum or the symptoms are mild, then you would not require any medication. However, changing your lifestyle to a certain extent can help you to take care of yourself. You may try out certain home remedies like
- Taking small bites of food and chewing carefully
- Drinking water during and after meals
- Sitting upright while eating your meals
- Eating a diet that is free of oil and spices
If there are worst conditions, then you would need a laparoscopic or esophageal diverticulum surgery to repair the esophageal lining
Esophageal Diverticulum Risk Factors
This disease esophageal diverticulum is usually uncommon and can be either congenital or acquired. This disease is known to occur in adults over 50- especially in people above 70 and older. There are no severe risks associated with the disease; however, individuals have an esophageal motility disorder like achalasia which causes malfunction of the sphincter muscles at the upper or lower end of the esophagus. People are at an increased risk of developing esophageal diverticula also.
by Dr. Christopher Chang, last modified on 1/7/17.
Read and comment below!
What is a Zenker’s diverticulum? (Click here to jump down to questions about treatment)
Zenker’s diverticulum is a pouch that forms at the back of the throat at the junction of the pharynx and the esophagus (the food passage to the stomach). The pouch causes problems with swallowing. In the image to the right, the arrow is pointing to the pouch.
Who gets a Zenker’s diverticulum?
Zenker’s diverticulum is most common in people over the age of 60. However, we have seen patients in their 30’s who have Zenker’s diverticulum.
What causes Zenker’s diverticulum?
The cause of Zenker’s diverticulum is not precisely known, though there are several hypothesis researchers have conjectured about. Some thoughts include reflux, baseline high cricopharyngeal muscle contraction, unusually weak posterior cervical esophageal wall, etc. It could also be a combination of factors. However, upon further study, none of these ideas have explained why some people develop it and others do not. The formation of the pouch does not appear to be hereditary. In many patients who have a Zenker’s diverticulum, other problems of the esophagus are present, though not always.
What are the most common symptoms of Zenker’s diverticulum?
The most common symptom of Zenker’s diverticulum is difficulty swallowing food. Food may actually come back up out of the mouth several minutes to even hours after eating. Patients also often complain of choking, feeling mucus collecting in the throat, hoarseness, or bad breath. The symptoms can be quite embarrassing and debilitating.
How is Zenker’s diverticulum diagnosed?
In patients with symptoms suggestive of Zenker’s diverticulum a very simple and safe x-ray called a Barium Swallow is performed. Upper endoscopy can also be used to diagnose a Zenker’s diverticulum, but for purposes of determining whether a patient is a surgical candidate, a barium swallow MUST be obtained.
How is Zenker’s diverticulum treated?
Surgery is required to effectively treat patients with Zenker’s diverticulum. We use a minimally invasive endoscopic treatment developed at Duke University known as Endoscopic Staple Diverticulostomy. Watch a slideshow or watch video. This treatment is safe, effective, and well tolerated. Dr. Chang has published articles in peer-reviewed journals and even wrote a book chapter describing this disorder and its treatments. There are other surgical methods which we do not generally advocate.
However, not all patients with Zenker’s Diverticulum are candidates for ESD. If the pouch is too small (
Symptoms of Esophageal diverticulum
Note that Esophageal diverticulum symptoms usually refers to various medical symptoms known to a patient, but the phrase Esophageal diverticulum signs may often refer to those signs that are only noticable by a doctor.
More Symptoms of Esophageal diverticulum:
More detailed symptom information may be found on the symptoms of Esophageal diverticulum article. In addition to the above medical information, to get a full picture of the possible signs or symptoms of this condition and also possibly the signs and symptoms of its related medical conditions, it may be necessary to examine symptoms that may be caused by:
- Complications of Esophageal diverticulum
- Hidden causes of Esophageal diverticulum
- Associated conditions for Esophageal diverticulum
- Risk factors for Esophageal diverticulum
- Related symptoms
Medical articles on signs and symptoms:
What are the signs of Esophageal diverticulum?
The phrase “signs of Esophageal diverticulum” should, strictly speaking, refer only to those signs and symptoms of Esophageal diverticulum that are not readily apparent to the patient. The word “symptoms of Esophageal diverticulum” is the more general meaning; see symptoms of Esophageal diverticulum.
The signs and symptom information on this page attempts to provide a list of some possible signs and symptoms of Esophageal diverticulum. This medical information about signs and symptoms for Esophageal diverticulum has been gathered from various sources, may not be fully accurate, and may not be the full list of Esophageal diverticulum signs or Esophageal diverticulum symptoms. Furthermore, signs and symptoms of Esophageal diverticulum may vary on an individual basis for each patient. Only your doctor can provide adequate diagnosis of any signs or symptoms and whether they are indeed Esophageal diverticulum symptoms.
by Gretchen Henkel • April 1, 2009
The condition can also lead to aspiration pneumonia. Symptoms can be present for several years before patients seek treatment.
You Might Also Like
Explore This Issue
The Gold Standard
Although endoscopic treatment of esophageal diverticula is now becoming standard of care (see sidebar), endoscopic-based diagnosis is not the usual strategy. The gold standard remains the barium swallow, asserted Dr. Postma.
Alexander T. Hillel, MD, a resident in the Department of Otolaryngology-Head and Neck Surgery at Johns Hopkins School of Medicine in Baltimore, who recently co-authored a historical review of endoscopic surgical management of ZD with Department Chair Paul W. Flint, MD, concurred with this approach: At our institution, when we are referred patients who are demonstrating symptoms of dysphagia and in whom a suspicion for esophageal diverticulum is high, we typically order a barium swallow.
But in the offices of Dinesh K. Chhetri, MD, Assistant Professor of Head and Neck Surgery and Director of the Swallowing Disorders Center at the David Geffen School of Medicine at the University of California, Los Angeles, patients with symptoms such as Mr. Landis’s might just as likely undergo fiberoptic endoscopic evaluation of swallowing (FEES) followed by transnasal esophagoscopy (TNE) to diagnose their problem.
During the January 2009 meeting of the Triological Society‘s Western Section, Dr. Chhetri and his research assistant Jennifer Long, MD, PhD, presented results of a retrospective cohort review, in which they reported that the finding of esophagopharyngeal reflux (EPR) when performing FEES has a high sensitivity and specificity for the presence of an esophageal diverticulum. TNE is then used to visualize and confirm the diagnosis of diverticulum during the same office visit, and the patient can be scheduled for surgery. I don’t find that the barium swallow is necessary anymore if I can diagnose the Zenker’s diverticulum in my office, Dr. Chhetri said recently from his Los Angeles office. With the knowledge that the pouch is there, I can then go ahead and schedule the patient for surgery.
Dr. Postma, who has published widely on the applications of FEES and TNE, said, When I do FEES and find an abnormality, very often it leads us to another diagnostic test. So, for example, if regurgitation occurs, that person is going to get a barium swallow. Many other conditions can account for the presence of EPR, he noted-including proximal esophageal strictures, severe esophageal dismotility, and tumors. Some small ZDs do not demonstrate EPR, and therefore would be missed if a barium swallow was not obtained. In addition, added Dr. Postma, obtaining a barium swallow allows me to look at the vertebral bodies for the presence of osteophytes. Large osteophytes sometimes make endoscopic exposure of a ZD more difficult.
by Gretchen Henkel • April 1, 2009
The FEES/TNE Diagnostic Process
Dr. Chhetri maintained that his methods for diagnosing diverticula offer a way to overcome what he calls the shortcomings of traditional radiologic evaluation-that is, diagnosis and treatment planning do not have to be delayed. Because many otolaryngologists now routinely perform FEES and TNE, they can more readily diagnose and plan treatment in one patient visit. (This may be more of an issue in private practice than at an academic center, where radiology is generally housed in the same building or on the same campus.)
You Might Also Like
Explore This Issue
When performing FEES, Dr. Chhetri first uses a 4% neosynephrine solution, without topical anesthetic, to decongest the nasal passages. After the scope has been passed along the floor of the nose and into the oropharynx, food mixed with green coloring is fed to the patient, beginning with puree, followed by nectar-thick, thin liquids, and a cookie. If patients are suspected to have a diverticulum, the endoscopist performs additional maneuvers to provoke EPR. These include asking the patient to phonate a sustained vowel (eeeee) after swallowing the food bolus and/or pressing on or massaging the patient’s anterior neck during sustained phonation. In his experience, said Dr. Chhetri, these maneuvers can cause the contents of a cervical esophageal diverticulum to be refluxed back to the hypopharynx. Observance of EPR would then lead Dr. Chhetri to perform TNE. After anesthetizing the nasal cavity with 4% lidocaine-soaked pledgets for several minutes, the transnasal esophagoscope is passed through the nasal cavity, advanced to the hypopharynx, and directed into a pyriform sinus, then allowed to pass into the cervical esophagus during a swallow.
If a ZD is present, the tip falls naturally into the diverticular pouch. Dr. Chhetri contended that he can generally estimate the pouch size by noting the distance the endoscope travels from the tip of the esophageal pouch to the level of the cricopharyngeal bar. After assessing the diverticulum, the scope is withdrawn to the cricopharyngeal bar and redirected toward the esophagus. The entire esophagus is then assessed all the way to the stomach.
Hindrance to Surgical Planning?
Dr. Hillel said that he recommends the standard barium swallow for definitive diagnosis and ease of surgical planning. So does Dr. Postma. The barium swallow gives you the ability to tell the size of the pouch-and size is pretty important, noted Dr. Postma. If the pouch is tiny, he explains, it may be impossible to insert the staple device used to perform the diverticulostomy. In the latter case, a laser myotomy is then performed.
How is a urethral diverticulum diagnosed?
Usually a urethral diverticulum is found during a routine pelvic exam or because a woman tells her doctor about symptoms she is having. At that point, the doctor does a physical exam or orders tests to try to find the cause.
In a physical exam, the doctor feels the vaginal wall to see if he or she can identify any masses, as well as to identify the location of any soreness. If he or she feels a sac, they may try to squeeze it gently to see if any built-up urine or pus comes out. The doctor would typically also order a urine analysis for a patient at this point.
If the exam leads the doctor to think there might be a problem, he or she can order imaging tests. These tests may include:
- Magnetic resonance imaging: Magnetic resonance imaging (MRI) is a test that produces very clear pictures, or images, of the human body without the use of X-rays. MRI uses a large magnet, radio waves, and a computer to produce these images. In patients who might have a UD, the MRI will look all around the pelvis but particularly around the vagina to see if there are any masses present.
- Ultrasound: This is a procedure that transmits high-frequency sound waves, inaudible to the human ear, through body tissues. The echoes are recorded and transformed into video or photographic images of the internal structures of the body. This can show the doctor if there are problems with the structures of internal organs around the vagina and if there is any swelling or build-up of urine.
- Urodynamic studies: These are a group of tests that can show a doctor how well the bladder, sphincters, and urethra hold and release urine. Used together or separately, as ordered by your doctor, these tests show how well the bladder works and can help explain why a patient is having leakage, pain, or other problems with urination. They typically involve injecting dye into the bladder and watching where it goes.
- Cystoscopy: This test involves looking into the urethra or bladder to see if one can identify a diverticulum and see the location of its opening. This is often done in the office.
Last reviewed by a Cleveland Clinic medical professional on 11/20/2016.
Zenker’s diverticulum is a pouch that forms at the back of the throat where the voice box (pharynx) and esophagus meet. The protruding pouch causes swallowing issues.
The primary symptom is difficulty in swallowing food; sometimes food comes back up several minutes or hours after eating.
People also experience:
- Choking feelings
- A feeling of mucous collecting in the throat
- Hoarse speech
- Bad breath
Tests for Diagnosing Zenker’s Diverticulum
Experts don’t know exactly what causes Zenker’s diverticulum, but do know it’s associated with increased pressure in the esophagus. This pressure causes the esophageal mucous membrane to herniate through a defective wall in the esophagus.
Some people with the disorder have other issues with their esophagus, but not always.
- Barium esophagography — provides an anatomic road for evaluation of the swallowing disorder.
- Upper endoscopy — examines the esophageal mucosa and helps identify conditions that may mimic Zenker’s diverticulum.
- Esophageal manometry — studies the pressure inside the esophagus.
Treating Zenker’s Diverticulum
UPMC thoracic surgeons perform both traditional and minimally invasive surgery for treating Zenker’s diverticulum.
Traditional surgery involves an open neck incision.
The minimally invasive technique uses a transoral (through-the-mouth) approach.
Compared to traditional open surgery, advantages to minimally invasive surgery for Zenker’s diverticulum include:
- Shortened hospital stay
- Quicker recovery time
- Earlier return to swallowing and eating normally
A diverticulum is an abnormal sac or pouch that develops at a weak point in the intestines. Various types of diverticula can develop as you age. When you’re born with a diverticulum in your intestines, it’s referred to as Meckel’s diverticulum.
Meckel’s diverticulum usually develops between the fifth and seventh weeks of fetal development. Because the condition is present at birth, it’s classified as a congenital health issue.
The symptoms of Meckel’s diverticulum are related to the type of diverticulum you have. In 95 percent of people with this condition, the diverticulum that develops is made up of intestinal cells. As a result, the diverticulum functions as a normal part of the intestine. This type of diverticulum may not cause any significant symptoms.
In other instances, the diverticulum may be made up of stomach or pancreatic cells. When this occurs, the diverticulum will function differently from the intestines. This may result in significant symptoms. These include:
- blockage of the intestines
- bleeding into the intestines, resulting in bloody stools
- inflammation in the intestines
- pain or discomfort that ranges from mild to severe
- nausea and vomiting
- anemia
Which symptoms you have often relates to how old you are when Meckel’s diverticulum is discovered. For example, infants with the condition are more likely to have a blockage in their intestines. Intestinal bleeding and bloody stools are more common in older children with the condition.
Most cases of Meckel’s diverticulum are identified and treated in children before the age of 10. The remaining cases are typically diagnosed in adolescence.
Meckel’s diverticulum may cause sporadic symptoms. When this occurs, you may notice blood in your stool for several days, followed by a period of normal stool. Erratic symptoms can make the condition difficult for your doctor to diagnose.
In rare cases, excessive bleeding from Meckel’s diverticulum may occur and become life-threatening. If this happens, emergency surgery may be needed to remove the diverticulum.
Talk to your doctor if you or your child has symptoms of Meckel’s diverticulum. They will recommend several different tests to confirm the diagnosis. Blood tests will determine if your red blood cell count is low. This will help your doctor determine if bleeding is occurring in the intestines. In addition, your doctor may order a stool smear. In this test, a sample of your stool is analyzed to see if it contains blood.
Your doctor may also order a technetium scan. This test uses a dye that can be viewed with a special camera. The dye will be injected into your veins and will collect around the diverticulum. This will help your doctor to see the pouch in your intestines. The results of this test can confirm the presence of Meckel’s diverticulum.
Some people may have active bleeding in their intestines as a result of Meckel’s diverticulum. This may make it difficult to view the diverticulum through the technetium scan. If this occurs, your doctor may need to order different tests to confirm diagnosis. A colonoscopy or upper gastrointestinal endoscopy may be ordered. These tests use a camera to visualize the diverticulum.
People who have Meckel’s diverticulum but don’t have any symptoms will not require treatment. Those who experience symptoms due to the condition may need to have surgery to remove the diverticulum. Surgery typically includes removal of the diverticulum and repair of the intestines.
If the intestines have been damaged as a result of the diverticulum, the damaged part of the intestine may also need to be removed. People who experience blood loss as a result of Meckel’s diverticulum may also require iron therapy or blood transfusions to replace lost blood.
Surgery to correct Meckel’s diverticulum is typically associated with a low risk of complications. However, some complications can arise following surgery. In particular, scar tissue may develop, which could cause a blockage of the intestines. Blockage of the intestines can be life-threatening and may require additional surgery to remove the blockage.
The long-term outlook for people who seek treatment for Meckel’s diverticulum is quite good. Surgical removal of the diverticulum typically results in normal intestinal function. Surgery also stops blood loss. People who have surgery for Meckel’s diverticulum can expect to make a full recovery.
Affiliations
- 1 1 Department of Surgery, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
- 2 2 Department of Surgery, The W.G. Hefner Veterans Medical Center, Salisbury, North Carolina.
- 3 3 Department of Surgery, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina.
- PMID: 31034339
- DOI: 10.1089/lap.2019.0239
Authors
Affiliations
- 1 1 Department of Surgery, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
- 2 2 Department of Surgery, The W.G. Hefner Veterans Medical Center, Salisbury, North Carolina.
- 3 3 Department of Surgery, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina.
- PMID: 31034339
- DOI: 10.1089/lap.2019.0239
Abstract
Introduction: Epiphrenic esophageal diverticula are typically treated with concurrent cardiomyotomy and diverticulectomy. However, resection of these diverticula can be technically difficult and associated with significant morbidity with a staple line leak rate ranging up to 27%. For this reason, and because the diverticulum is secondary to a primary esophageal motility disorder such as achalasia, we decided to adopt a laparoscopic myotomy-first strategy, reserving the diverticulectomy for patients with persistent or recurrent symptoms. Methods: From 2004 to 2018, 22 patients with epiphrenic diverticula were treated by laparoscopic Heller myotomy and partial fundoplication alone, with the plan to add the diverticulectomy as a second stage if needed. There were 13 women and 9 women, with a mean age of 68 years. Results: Patients had been symptomatic for an average of 36 months. The most common presenting symptom was dysphagia (91%), followed by regurgitation (77%). More than half of the diverticula were solitary and on the right side. Esogphagoscopy ruled out cancer. Esophageal manometry (18 patients) showed achalasia in 14 patients, nutcracker esophagus in 3 patients, and nonspecific motility disorder in 1 patient. There were no perioperative complications, and average length of stay was 2.5 days. At a mean follow-up of 68 months, dysphagia resolved in 77% and regurgitation in 86% of patients. Three patients had persistent symptoms: 2 patients underwent a transthoracic diverticulectomy (1 patient with resolution of symptoms and 1 patient with no improvement). Another patient had per oral endoscopic myotomy, but his dysphagia persisted. Conclusions: The laparoscopic myotomy-first approach reduces risk and unnecessary surgery. A laparoscopic Heller myotomy and partial fundoplication provide excellent resolution of symptoms for most, whereasonly a few will need a staged resection of the diverticulum.
Keywords: achalasia; diverticulectomy; epiphrenic diverticulum; esophageal motility disorders; laparoscopic Heller myotomy; partial fundoplication.
What is Zenker’s Diverticulum?
Zenker’s diverticulum (ZD) is a condition characterized by a pouch that develops in the upper esophagus in the neck. The pouch can contain food which can cause difficulty or pain with swallowing and bad breath. Cases of ZD are generally categorized as small, intermediate, or large, depending on the size of the pouch. The condition appears more often in men and women older than 50, and affects men more frequently than women.
Treatment of Zenker’s Diverticulum requires an interdisciplinary approach that draws on various medical specialties. At BMC, physicians in our Center for Minimally Invasive Esophageal Therapies provide comprehensive, quality care including medical oncology, radiation oncology, thoracic surgery, gastroenterology, pathology, pulmonary medicine and radiology.
What are the Symptoms of Zenker’s Diverticulum?
Symptoms may include:
- Discomfort with swallowing
- Regurgitation of undigested food hours after eating
- Coughing or the feeling of food sticking in the throat after eating
- Aspirating food or liquid that enters the airway and causes choking or bleeding
- Bad breath
- Unexplained weight loss
What are the Causes?
The cause is most commonly secondary to increased tension in the muscle at the top of the esophagus (called the cricopharyngeus muscle) causing a functional obstruction.
How is Zenker’s Diverticulum Diagnosed?
ZD is generally diagnosed by means of a [shortcode-diagnostics-Barium-Swallow]
Other tests your physician may prescribe for you include:
Endoscopy
You will receive an intravenous sedative and pain medication. Once comfortable, the physician will then examine the area using an endoscope—a lighted tube with a small camera at the end. The physician will be able to view any abnormalities and take a tissue samples (biopsies) if necessary.
Esophageal Manometry
This test measures the pressure inside the lower esophageal sphincter (LES). A thin tube is inserted through your mouth or nose and into your stomach. Once it is in place, the physician will gently pull the tube back into the esophagus and ask you to swallow. As you do so, the pressure and coordination of your muscle contractions will be measured. If the pressure is low or the LES is not relaxing properly, achalasia may be present. If the pressure is low or the LES is not contracting properly, it may indicate GERD (reflux disease).
A physical examination and patient history are also important parts of diagnosis.
How is Zenker’s Diverticulum Treated?
There are currently no medications to treat ZD. Surgery is the main therapeutic approach; however, some small diverticula do not require treatment. Open and endovascular or transoral repair have both been found to be successful.
For open surgery, an incision is made in your neck and the pouch is removed or tacked upside down so it cannot fill—or it is removed completely. An important part of the operation is to cut the muscle just below the diverticulum to prevent recurrence. Most patients must stay in the hospital for one or two days after the procedure.
In endoscopic repair or transoral repair, a stapling device is inserted through the mouth using metal tubes. The muscle between the pouch and the esophagus is divided, thereby making the pouch part of the upper esophagus. This method does not require an incision, is faster, equally effective and reduces the risk of complications, as well as time in the hospital.
Your physician will work with you to determine the best treatment option, according to your unique situation.
(Esophageal Diverticula)
Kristle Lee Lynch
, MD, Perelman School of Medicine at The University of Pennsylvania
The cause depends on the type of diverticula.
Symptoms include spitting up of food and difficulty swallowing.
The diagnosis is based on the results of barium swallow x-rays and often upper endoscopy.
When needed, treatment includes surgery.
The esophagus is the hollow tube that leads from the throat (pharynx) to the stomach. (See also Overview of the Esophagus.)
There are several types of esophageal diverticula. Each has a different cause, but probably all are related to uncoordinated swallowing and muscle relaxation. Many of these diverticula are associated with motility disorders of the esophagus, such as esophageal spasm and achalasia.
Zenker diverticula (pharyngeal diverticula)
A Zenker diverticulum is probably caused by an incoordination between movement of food out of the mouth and relaxation of the cricopharyngeal muscle (cricopharyngeal incoordination). This diverticulum can fill with food, which may be spit up (regurgitated) when the person bends over or lies down. This regurgitation may also cause food to be inhaled into the lungs during sleep, resulting in aspiration pneumonia. Rarely, the pouch becomes larger and causes difficulty swallowing (dysphagia) and sometimes a swelling in the neck.
Midesophageal diverticula (traction diverticula)
A midesophageal diverticulum is caused by inflammation located in the chest cavity outside the esophagus that pulls on the esophagus or is caused by esophageal motility disorders. A midesophageal diverticulum rarely causes symptoms, but the underlying motility disorder may.
Epiphrenic diverticula
An epiphrenic diverticulum occurs just above the diaphragm (the muscle that separates the chest from the abdomen) and usually occurs along with a motility disorder (such as achalasia or esophageal spasm). An epiphrenic diverticulum rarely causes symptoms, but the underlying motility disorder may.
Diagnosis
Barium swallow x-rays
Often upper endoscopy
Doctors diagnose all types of esophageal diverticula by doing a barium swallow (esophogram). In this test, people are given barium in a liquid before x-rays are taken. The barium outlines the esophagus, making abnormalities easier to see. Sometimes the barium swallow is videotaped so doctors have a recording of it.
Doctors often do an upper endoscopy to confirm the diagnosis. During upper endoscopy, doctors examine the esophagus by using a flexible tube called an endoscope.
Treatment
Usually no treatment
Treatment of diverticula is not usually needed.
If symptoms are severe or the pouch is large, however, the pouch can be removed surgically.
Diverticula associated with motility disorders require treatment of the underlying disorder. For example, if a Zenker diverticulum is caused by an abnormally functioning cricopharyngeal muscle, a doctor can cut the muscle (a procedure called myotomy) when removing the Zenker diverticulum.
How are esophageal varices diagnosed?
Regular screening for esophageal varices is recommended for people who have advanced liver disease. Screening is done by endoscopy. An endoscope is a thin, flexible tube with a light and a tiny camera on the tip. The physician passes the endoscope down the esophagus, and the camera sends images of the inside of the esophagus to a monitor. The physician looks at the images to detect enlarged veins and grades them by size. Red lines on the veins are a sign of bleeding.
The physician may also use the endoscope to examine the stomach and the upper part of the small intestine. This is called an esophogastroduodenoscopy (EGD).
Imaging by CT or MRI scan is also used to diagnose esophageal varices, often in combination with endoscopy. The pictures created by CT or MRI show the esophagus, the liver and the portal and splenic veins. They give the physician more information about the liver’s health than endoscopy alone.
Last reviewed by a Cleveland Clinic medical professional on 04/10/2019.
References
- Garcia-Tsao G, Sanyal AJ, Grace ND, Carey WD. Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis. Am J Gastroenterol 2007;102:2086–2102.
- Poza Cordon J, Froilan Torres C, Burgos García A, et al. Endoscopic management of esophageal varices. World Journal of Gastrointestinal Endoscopy. 2012 Jul 16;4(7):312-22.
- Merck Manual Consumer Version. Gastrointestinal Bleeding. Accessed 4/17/2019.
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Esophageal dysphagia typically results from a motility disorder or a physical obstruction that prevents food and drink from passing easily through the esophagus. Motility disorders and obstructions that lead to esophageal dysphagia include:
- A narrowing of the esophagus (strictures)
- Gastroesophageal reflux disease (GERD)
- Eosinophilic esophagitis (EoE)
- Achalasia or other motility disorders such as Jackhammer esophagus
- A benign or cancerous growth or blockage
- Zenker’s diverticulum
Esophageal dysphagia is diagnosed with a variety of tests, and can often be alleviated with minimally invasive surgical or endoscopic procedures.
Please check your filter options and try again.
Tests for Esophageal Dysphagia
If you experience difficulty swallowing, frequent coughing or gagging while eating, or feel like food is stuck in your throat, your doctor may recommend one or more of the following tests to determine the severity of your dysphagia.
Barium Swallow
A barium liquid is swallowed and travels the length of your esophagus. X-ray images show how food and liquid travel through your esophagus.
Upper Endoscopy (EGD)
Your doctor inserts a flexible tube into your mouth to view the inside of your esophagus, stomach, and small intestine.
Esophageal Manometry
A tiny electronic device is inserted into your nose and guided to your esophagus via a thin, flexible tube called a catheter. It evaluates motility by monitoring strength and patterns of muscle function within the esophagus.
EndoFLIP
During endoscopy, your gastroenterologist uses a device to measure pressures inside your esophagus and assess esophageal motility.
Duke Health offers locations throughout the Triangle. Find one near you.
Dysphagia Treatments
Medical Management
Medications may be prescribed to reduce acid production and relax the esophageal muscles. Antibiotics may be prescribed for esophageal infections.
Esophageal Dilation
During an endoscopy, a balloon is passed into the esophagus. The balloon is then inflated to stretch narrowed areas that impede swallowing. Another type of dilation procedure uses a dilator passed through the esophagus during an endoscopy. This is performed as an outpatient procedure.
Heller Myotomy
During this minimally invasive procedure, your surgeon makes several small incisions and passes small surgical instruments through a laparoscope to reach the esophagus. Small cuts are made in the esophageal muscle to relieve pressure. If necessary, your surgeon may also wrap part or all of the stomach around the lower esophagus to strengthen the muscle. This is called a fundoplication.
POEM (Per-oral Endoscopic Myotomy)
This minimally invasive procedure helps people with achalasia eat and drink comfortably again. An endoscope is passed through the mouth and into the esophagus. This allows doctors to see and cut the esophageal muscle that cause the swallowing disorder. There are no surgical incisions.
Endoscopic Diverticulotomy
If you have moderate to severe Zenker’s diverticulum, your surgeon may use an endoscope to reach the esophagus and remove or change the position of the pouch that is causing your swallowing discomfort.
Esophageal Stent Placement
If your esophagus is partially blocked or narrowed, your doctor will use a small cylinder called a stent to open the esophagus and ease your symptoms. This procedure is performed through an endoscope.
Why Choose Duke
Extensive Experience
Our gastroenterologists have completed specialized training and are highly skilled in the use of endoscopy to diagnose dysphagia and other esophageal motility disorders. Our board-certified surgeons have additional fellowship training in thoracic surgery. This includes specialized procedures in and around the esophagus.
A Team of Specialists for Your Condition
Because dysphagia can result from many different conditions, a team of experts from different specialties may be involved in your care. This may include highly trained, board-certified speech pathologists and otolaryngologists, as well as gastroenterologists and neurologists. We work together to ensure you receive the best treatment for your condition.
More Complex Procedures
If your condition requires surgery, you may benefit from our use of robot-assisted surgery, which allows our surgeons to visualize the surgical site better. The precision of the robotic tools allows our doctors to do more complex procedures in smaller areas and place sutures with greater accuracy.
Research Advances
Our specialists have made major contributions that have improved treatment and outcomes for people with esophageal dysphagia, and conduct clinical trials to uncover better treatment options. For example, Duke doctors pioneered endoscopic staple diverticulostomy (ESD), the first minimally invasive surgery for Zenker’s diverticulum.
A thorough and accurate cancer diagnosis is the first step in developing an esophageal cancer treatment plan. Your care team will use a variety of tests and tools designed for diagnosing esophageal cancer, evaluating the disease and developing your individualized treatment plan. Throughout your treatment, we’ll use imaging tests to track the size of the tumors, monitor your response to treatment, and modify your plan when needed.
Examples of procedures used for diagnosing esophageal cancer include:
Advanced genomic testing examines a tumor to look for DNA alterations that may be driving its growth and other behaviors. By identifying the mutations that occur in a cancer cell’s genome, we may be able to tailor your treatment based on these findings.
Nutrition panel is used to evaluate patients for deficiencies in nutrients, such as vitamin D and iron. The test may help identify the nutrients patients need replaced or boosted to support their quality of life. Learn more about our nutrition therapy program.
Upper endoscopy is one of the most common ways of diagnosing esophageal cancer. It may be used as a biopsy, as well as to determine the extent of the tumor. The camera on the end of the endoscope allows doctors to see the lining of the esophagus and detect abnormalities. The procedure is performed while the patient is under sedation.
Biopsy may not only be used to help diagnose cancer, but it also may help differentiate an adenocarcinoma from squamous cell carcinoma, which are two types of esophageal cancer with very different treatments and prognoses.
Endoscopic ultrasound (EUS) allows doctors to see the esophagus and surrounding tissues on an ultrasound machine. This test for esophageal cancer is designed to detect abnormalities in the surrounding tissue and lymph nodes. An EUS also helps stage esophageal cancer, which guides treatment decisions and prognosis assessments.
CT scan for esophageal cancer uses X-ray images to present detailed images of the esophagus and surrounding tissues. It also helps to identify the spread of cancer to other distant organs, such as the liver. The GE Discovery™ PET/CT 600 Scanner is a four-dimensional CT scanner that produces detailed cross-sectional X-ray images of structures within the body. It also enables our radiologists to plan treatment around patients’ breathing patterns.
Magnetic resonance imaging (MRI) may be useful in detecting esophageal tumors and metastases. This diagnostic technique offers greater soft tissue contrast than a CT scan.
ET/CT scans are designed to detect cancer, no matter where it is located in the body, sometimes before tumors or structural changes in the esophagus develop.
What is Zenker’s Diverticulum?
Zenker’s diverticulum (pharyngeal pouch/hypopharyngeal diverticulum/ pharyngoesophageal diverticulum) is a diverticulum which is formed from the mucosa of the pharynx and is situated above the cricopharyngeal muscle, which is present above the upper sphincter of the esophagus. Zenker’s diverticulum is a false diverticulum, as it does not involve all the layers of the esophageal wall. Zenker’s diverticulum was named by Friedrich Albert von Zenker, who was a German pathologist, in 1877.
Causes of Zenker’s Diverticulum
The main cause of Zenker’s Diverticulum is thought to be malfunctioning of the cricopharyngeal muscle due to the aging process. Neurologic medical conditions, such as a stroke, also can cause malfunctioning of the cricopharyngeal muscle. Excessive pressure in the lower pharynx causes ballooning out of the weakest part of the pharyngeal wall resulting in formation of diverticulum, which can be many centimeters in diameter.
According to current research, occlusive mechanisms are thought to play an important role in formation of Zenker’s Diverticulum, such as impaired relaxation, uncoordinated swallowing, and spasm of the cricopharyngeus muscle; all these things lead to increased pressure in the distal pharynx which leads to its herniation through the point of least resistance. This point is known as Killian’s triangle, which is situated superior to the cricopharyngeus muscle and lower to the inferior constrictor muscles. This causes outpouching of the posterior pharyngeal wall, which is just above the esophagus.
Signs & Symptoms of Zenker’s Diverticulum
Zenker’s diverticulum can be asymptomatic; however, the following symptoms can be present:
- Dysphagia (difficulty swallowing) with a feeling of lump in the throat.
- Food can get trapped in the outpouching, which can cause regurgitation which is the reappearance of ingested food in the mouth).
- Pain can be experienced very rarely.
- Halitosis, which is bad breath, due to stagnant food being digested by microorganisms.
- Cough can occur due to the regurgitated food into the airway.
- Infection.
- Cervical webs can be seen in half of the patients with this condition.
- Feeling of a lump in the neck.
- Involuntary gurgling noises when the patient is swallowing.
- Hoarseness (changes in voice).
- Pneumonia can occur due to aspiration of the food present in the windpipe.
- Share
- Feedback
Medical Care
Asymptomatic and minimally symptomatic esophageal body diverticula do not require treatment.
In many patients with mid esophageal and epiphrenic diverticula, dysphagia is related to underlying dysmotility; thus, treatment should be directed to the motility disorder when feasible. For instance, achalasia can be treated with pneumatic dilation, botulinum toxin injection into the lower esophageal sphincter, or surgical Heller esophagomyotomy.
Treatment of esophageal intramural pseudodiverticulosis is directed toward underlying strictures or dysmotility.
Surgical Care
Treatment of Zenker diverticulum traditionally has been surgical, although the specific operation used still is controversial. Surgical options include diverticulectomy with cricopharyngeal myotomy, diverticular suspension (diverticulopexy) with cricopharyngeal myotomy, and cricopharyngeal myotomy alone.
Diverticulectomy
Consider diverticulectomy when esophageal body diverticula are believed to be the cause of aspiration. An abdominal laparoscopic approach may be feasible for some patients with epiphrenic diverticula. Case reports of endoscopic treatment of giant midesophageal diverticula have been reported. However, patients who are being considered for diverticulectomy should first undergo careful study with barium swallow, flexible endoscopy, and esophageal manometry. Treatment directed at an underlying esophageal motility disorder, such as achalasia, cannot be ignored.
Diverticulectomy usually is not performed by itself, because it does not correct the defect in cricopharyngeal function that usually contributes to the formation of a Zenker diverticulum. While the transcervical approach has been used traditionally, the transoral route using a rigid esophagoscope also may be used.
Good results have been obtained by performing a diverticulotomy using a flexible endoscope and needle-knife papillotome to cut the common wall between the diverticulum and the oropharynx as well as the cricopharyngeus while the patient is consciously sedated. Data suggest that this technique offers good results with a relatively high success rate, but it should be performed in large centers with surgeons who are experienced with this technique. In some variations of this technique, the diverticulum is stapled. [12]
Other procedures
Other novel techniques are being developed. Flexible endoscopic diverticulotomy approaches have been explored using various techniques, including argon plasma coagulation, monopolar coagulation forceps, and needle-knife incision. [9, 10, 13, 14] These techniques typically use a cap or hood attached to the endoscope. The goal of these techniques is the division of the septum between the diverticulum and the esophagus, thus performing a cricopharyngeal myotomy.
Increased efforts to a laparoscopic approach to repair both epiphrenic diverticula and Zenker diverticula have been explored. The literature supports open surgery and a laparoscopic approach as appropriate methods of repair. [15] The laparoscopic technique uses stapler closure, and multiple case reports cite wound leakage from stapler failure as a complication. With complication rates as high as 20%, a skilled surgeon with experience in this procedure is beneficial. Benefits of the laparoscopic approach include decreased morbidity because of no thoracotomy wounds and chest tubes and a less invasive approach.
A study of 229 endoscopic diverticulotomies (in 189 patients), conducted by Kos et al, indicated that better results can be achieved using a combination of CO2 laser and Acuspot in the endoscopic procedure than by employing endoscopic diverticulotomy with electrocautery or with a carbon dioxide (CO2) laser alone. [9] The investigators reported the following postsurgical results:
Endoscopy with CO2 laser: Dysphagia was absent following 78.4% of procedures; repeat surgery was required following 19.6% of procedures
Endoscopy with electrocautery: Dysphagia was absent bsent following 72% of procedures; repeat surgery was required following 24.3% of procedures
Endoscopy with CO2 laser and Acuspot: Dysphagia was absent following 84.6% of procedures; repeat surgery was required following 13% of procedures
Several reports in the literature lately describe surgical treatment of esophageal diverticula. One recent publication analyzed a single surgeon’s experience with endoscopic CO2 laser and stapler repair of Zenker diverticulum by comparing dysphagia and regurgitation outcomes in 148 patients. This report concluded that endoscopic CO2 laser and staple methods are effective in treating Zenker diverticulum. The laser can have greater efficacy and result in lower recurrence rates. [16]
Most of the reports involve treatment of Zenker diverticula and discuss open versus endoscopic methods. [17, 18, 19, 20] None was a controlled study. They were series reports or retrospective reviews. There is no consensus of which method is the best.
- Share
- Feedback
Laboratory Studies
Most laboratory studies are not helpful in the diagnosis. (Upper esophageal webs have been associated with iron deficiency anemia.)
Imaging Studies
Radiographic studies and upper GI endoscopy detect many esophageal diverticula incidentally because esophageal diverticula often are asymptomatic. On standard chest radiographs and CT scans, large diverticula of the esophagus and hypopharynx also may manifest as air-filled and/or fluid-filled structures communicating with the esophagus.
Barium radiography (ie, barium esophagography, barium swallow) generally is the diagnostic procedure of choice. In addition to being excellent at defining the structural appearance of diverticula, barium swallow also may provide clues to underlying motility disturbances that may be involved in diverticular formation. However, if the patient has dysphagia or odynophagia or has alarm symptoms, then upper endoscopy is indicated.
Barium swallow is a useful study in patients who are symptomatic and have mid esophageal and epiphrenic diverticula. Diagnosis of esophageal intramural pseudodiverticulosis is made best using barium radiography. Diagnosis of Zenker diverticulum is made best using barium swallow, which should include lateral views of the pharyngoesophageal junction. It also can be made using careful upper endoscopy by an experienced endoscopist.
Some reports have described Killian-Jamieson diverticula being detected on ultrasonography of the thyroid gland. [4] Because of the proximity of the upper esophagus to the thyroid gland, pharyngoesophageal diverticula may mimic thyroid nodules on thyroid ultrasonography. [5] A Zenker diverticulum reportedly can be distinguished from a thyroid nodule on ultrasound by the sign of air in the diverticulum. [6]
Pharyngeal and esophageal diverticula, rings, and webs : GI Motility .
Esophageal diverticulitis are pockets formed in your esophagus that can trap food and . The doctor will lower a tube down your throat to examine what types of .
Esophageal Diverticulum: Symptoms, Causes, Diagnosis, and Treatment
Learn more about Zenker’s throat where the voice box .
Are there alternatives to surgery for Zenker diverticulum? | Cleveland .
Esophageal Pouches (throat (pharynx) to the stomach.
Esophageal Diverticulum | Cleveland Clinic
diverticulitis, fatigue, swollen lymph nodes) but then it may go into an .
Zenker’s diverticulum – Wikipedia
A Zenker’s diverticulitis; Food might get trapped in the outpouching, leading to:.
Zenker’s Diverticulum – Temple Head & Neck Institute – Philadelphia .
Find out how the Esophageal Center treats esophageal throat, a condition in which parts of the esophagus become weakened.
Diverticulitis: Symptoms, Causes, Diagnosis, Treatment
Conventional treatment for a large symptomatic Zenker throat is to surgically either remove it (diverticulectomy) or obliterate it by repositioning and .
Esophageal Diverticula Treatment & Management: Medical Care .
Symptoms of esophageal diverticulitis; Heartburn; Regurgitation (the return of partially digested food from the .
Esophageal Diverticulum | Cleveland Clinic
Zenker’ s diverticulitis, above the cricopharyngeal muscle. This muscle can malfunction resulting in neurologic .
Zenker’s Diverticulum – Texas Ear, Nose & Throat Specialists Texas .
Zenker’s diverticulitis is dysphagia, or difficulty swallowing.
Zenker’s Diverticulum | Conditions We Treat | Boston Medical Center
G&H What are the various manifestations of esophageal throat symptoms, so that it .
Esophageal Diverticula Symptoms | Northwestern Medicine
Q: What is an esophageal diverticulitis to the stomach. . Symptoms may include difficulty swallowing (dysphagia), chronic coughing .
Esophageal diverticula – Cancer Therapy Advisor
Zenker’s diverticulitis ) pressure due to fibrosis of the upper esophageal sphincter.
Zenker’s Diverticulum – Diagnosis & Treatment – UPMC.com
Zenker’s throat after eating .
Esophageal Diverticula – Cedars-Sinai
Zenker’s diverticulitis may also be .
Esophageal Diverticula – NCBI – NIH
An esophageal diverticulitis, in the mid-chest.
Esophageal Pouches (Diverticula) – Digestive Disorders – Merck .
Esophageal throat and are the result of .
3 Ways to Treat Esophageal Diverticulum – wikiHow
A Zenker’s throat typically arises due to tightness of the cricopharyngeus muscle. This muscle makes up the upper esophageal sphincter, and is located just below the level of the voice box. Normally, it relaxes during swallowing to allow food to pass into the esophagus.
Zenker’s Diverticulum
What is Zenker’s diverticulum?
The esophagus, the muscular tube that connects the throat and the stomach, has a muscular sphincter at its upper end that controls the passage of food into the stomach. This upper esophageal sphincter (UES)—also called the cricopharyngeus—is a semi-circular muscle located in the neck about three inches below the Adam’s apple. To prevent the reflux of foods from the esophagus into the throat, the cricopharyngeus remains contracted and tight at most times. When a person swallows, though, it relaxes and allows food to pass through. If the muscle doesn’t relax, and food is blocked from passing into the esophagus (a condition called cricopharyngeal dysfunction), the food can push down on the muscle with enough pressure to stretch it and create a sac called a diverticulum. When a patient swallows, the food will get stuck in that sac.
What are the symptoms of Zenker’s diverticulum?
Patients with Zenker’s diverticulum have difficulty swallowing, and describe food sticking and a sensation of fullness in the neck. They may have no problem swallowing liquids, but often have difficulty swallowing solid foods. Often, 20 to 30 minutes after attempting to swallow, they’ll cough out undigested food.
How is Zenker’s diverticulum diagnosed?
Physicians diagnose Zenker’s diverticulum using a test called a barium swallow. During this test patients are asked to swallow a variety of substances that are coated with barium, a whitish paste that lights up during an X-ray, enabling the radiologist to determine how well these substances are moving through the mouth, pharynx, and esophagus. The test will show if the upper esophageal sphincter is not relaxing or if foods or liquids are blocked as they pass through the esophagus. If a Zenker’s diverticulum is present, physicians can see the outline of the sac.
How is Zenker’s diverticulum Treated?
Physicians treat Zenker’s diverticulum when it significantly affects a patient’s quality of life, or causes him or her complications such as aspiration pneumonia. The diverticulum can be treated surgically using one of two approaches. Physicians can perform the procedure through an incision made on the outside of the neck (transcervically), then remove the sac completely. More recently a minimally invasive transoral approach has become the treatment of choice. This is an endoscopic procedure in which a physician cuts the wall that separates the sac from the esophagus. Food that goes into the sac will then flow right into the esophagus. Patients treated with this newer approach have less discomfort and a faster recovery but may have slightly higher chance of a recurrence.
What is the outlook for people with Zenker’s diverticulum
Patients who are treated for Zenker’s diverticulum have an excellent prognosis, and most patients become free of any swallowing difficulty. A small number of patients (about 20%) continue to experience some difficulty swallowing, but it does not affect their well-being. A much smaller number of patients (3% to 7%) have a recurrence of symptoms and their diverticulum and will likely need to be re-treated.
Make an Appointment
Adult: 212-305-8555
Pediatric: 212-305-8933
For more information,
visit our contact us page.
Affiliation
- 1 Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine.
- PMID: 30834217
- PMCID: PMC6383851
- DOI: 10.5090/kjtcs.2019.52.1.40
Free PMC article
Authors
Affiliation
- 1 Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine.
- PMID: 30834217
- PMCID: PMC6383851
- DOI: 10.5090/kjtcs.2019.52.1.40
Abstract
Epiphrenic diverticula are known to cause a series of complications. We report the case of a 54-year-old woman who was diagnosed with an epiphrenic diverticulum at a regular checkup in November 2006. Ten years later, she presented with massive hematemesis. Imaging studies revealed an epiphrenic diverticulum measuring 7.8 cm in diameter and a large amount of bleeding inside the diverticulum. Computed tomography showed fistula formation between the diverticulum and the left lower lobe of the lung, leading to the development of a pulmonary abscess. Diverticulectomy and 180° posterior partial fundoplication were performed transabdominally. The pulmonary abscess was treated with antibiotics alone. She was discharged 16 days after the operation without any complications over 7 months of follow-up.
Keywords: Esophageal diverticulum; Esophagopulmonary fistula.
Conflict of interest statement
Conflict of interest No potential conflict of interest relevant to this article was reported.
Figures
An esophagogastroduodenoscopic examination revealed a…
An esophagogastroduodenoscopic examination revealed a large hematoma inside the diverticulum.
An esophagographic examination showing an…
An esophagographic examination showing an epiphrenic diverticulum on the left side of the…
(A) An image from a…
(A) An image from a lung-window chest computed tomography scan shows an epiphrenic…
An image of esophagography on…
An image of esophagography on postoperative day 1, using gastrograffin.
An image from a mediastinal-window…
An image from a mediastinal-window chest computed tomography scan on postoperative day 65,…
, VMD, DACVIM, DACVECC, New England Animal Medical Center
Diverticula are pouch-like dilatations of the esophageal wall and may be congenital or acquired. They are rare in dogs and cats. Acquired diverticula are of two types: pulsion or traction. Pulsion diverticula are caused by increased intraluminal pressure or deep esophageal inflammation, which can lead to mucosal herniation. Predisposing conditions include esophagitis, esophageal stricture, foreign bodies, vascular ring anomalies, megaesophagus, and hiatal hernia. This type of diverticulum involves the esophageal epithelium and connective tissue. Traction diverticula result from inflammation in the chest cavity in close proximity to the esophagus. Fibrous tissue is produced, which then contracts, pulling the esophageal wall outward. This diverticulum involves all layers of the esophagus.
Small diverticula may be subclinical. Large diverticula allow food to become trapped in the pouch, leading to postprandial dyspnea, regurgitation, and anorexia. Survey radiographs may show the diverticulum if it is full of ingesta or air, but contrast radiographs are best to demonstrate the pouch. Endoscopy will also allow visualization and can identify ulceration and scarring.
Small diverticula may be treated with a bland, soft diet fed with the animal in an upright position. Large diverticula require surgical excision and reconstruction of the esophageal wall. The prognosis after surgery is fair to good.
Ulcers are sores or lesions that commonly occur along the upper digestive tract. When they form in this area, they are known collectively as peptic ulcers.
Individually, peptic ulcers are described by where they are found, the most common being gastric ulcers in the stomach and duodenal ulcers in the upper portion of the small intestine.
Peptic ulcers that occur in the esophagus are known as esophageal ulcers.
In this article, we explore the details of esophageal ulcers, including their symptoms, causes, and the available treatments.
Fast facts on esophageal ulcers
- They are a type of peptic ulcer that develops in the lining of the esophagus, the tube that connects the throat to the stomach.
- Symptoms include pain or a burning sensation behind or below the sternum, the flat bone that runs down the center of the chest.
- Medications, infections, and exposure to stomach acid are common causes.
- Treatment involves addressing the cause of the ulcer.
An esophageal ulcer is a type of peptic ulcer that develops in the lining of the esophagus, the tube that connects the throat to the stomach.
Esophageal ulcers occur when the layer of mucus, which lines and protects the gastrointestinal tract, wears away.
This allows stomach acid and other gastric juices to irritate the gastrointestinal wall, leading to ulceration.
Aside from a burning pain in the center of the chest, esophageal ulcers typically cause pain or a burning sensation behind or below the sternum, in the center of the chest.
Other symptoms include:
- loss of appetite
- difficulty swallowing
- heartburn
- nausea
- shortness of breath
- sore throat
- sour taste in the mouth
- abdominal pain
- vomiting, sometimes including blood
- weight loss
The main causes of esophageal ulcers are:
Exposure to stomach acid: This causes chronic inflammation and irritation of the esophagus, allowing ulcers to develop. Stomach acid exposure most often occurs in people with other gastrointestinal conditions. These can include hiatal hernias and GERD, or gastrointestinal reflux disease, more commonly referred to, as severe heartburn.
Medications: Certain drugs, including aspirin, ibuprofen, bisphosphonates, and some antibiotics, can cause esophagitis, or inflammation of the esophagus, and esophageal ulcers.
Infection: Ulcers caused by infection are less common, but the fungal infection known as candida, herpes, and the human papillomavirus (HPV) have all been linked to esophageal ulcers.
Caustic injury: Esophageal ulcers may be caused by ingesting a corrosive substance. This type of injury mostly affects children, but it can also occur in adults who experience psychosis, suicidal tendencies, or who are abusing alcohol.
Certain types of gastric surgery or foreign bodies can also cause esophageal ulcers.
Early intervention is key to preventing complications from esophageal ulcers.
In cases of acid reflux, treatment may include:
- Medication, such as antacids, H-2-receptor blockers, and proton pump inhibitors (PPIs).
- Dietary and lifestyle changes, to aid digestion.
- Surgery, for severe cases. Types of surgeries include to tighten the LES (lower esophageal sphincter) valve near the top of the stomach or to insert a magnetic device to help the LES valve function.
Esophageal ulcers that are not caused by GERD may require different interventions. For example, antibiotics or antifungals may be prescribed in cases of ulcers caused by infection.
Making changes to lifestyle and diet can be beneficial in reducing acid reflux and GERD, which are common causes of esophageal ulcer formation.
Lifestyle and dietary changes
Lifestyle changes to treat ulcers include:
- eating slowly
- never overeating
- avoiding lying down for approximately 3 hours after eating
- maintaining a healthy body weight
- wearing loose clothing to reduce pressure on the stomach
- quitting smoking, as smokers are at greater risk of GERD
- raising the head of the bed to reduce nighttime acid reflux
Dietary changes to treat ulcers include eating a balanced diet of lean protein, whole grains, nuts, seeds, fruits, and vegetables.
Certain foods and drinks trigger GERD and should be avoided. They include:
- alcohol
- caffeine
- chocolate
- citrus
- fried foods
- garlic
- high-fat foods
- mint
- onions
- spicy foods
- tomatoes and tomato-based foods
Since foods that trigger acid reflux and GERD can vary between individuals, it can be helpful to keep a diary of daily food intake and associated symptoms.
Zenker’s Diverticulum – a sac or pouch in the back of the throat which causes difficulty swallowing by collecting and retaining food and saliva.
Zenker’s Diverticulum – a sac or pouch in the back of the throat which causes difficulty swallowing by collecting and retaining food and saliva.
Symptoms of a Zenker’s Diverticulum:
- Regurgitation of undigested food
- Difficulty swallowing
- Feeling of pills stuck in throat
- Coughing while eating
- Choking on foods
- “Lump in the throat” sensation
- Increased phlegm
Cause of Zenker’s Diverticulum
The cricopharyngeus muscle is located at the bottom of the throat. This muscle is normally contracted, to prevent reflux, or the flow of food and acid backwards from the esophagus into the throat. When this muscle is overactive, the tissue above it stretches and dilates. This dilation turns into a pouch in the back of the throat known as a Zenker’s Diverticulum. Food, pills and saliva get stuck in the Zenker’s diverticulum while swallowing.
Diagnosis
Laryngoscopy is the first step to evaluate the throat and examine for abnormalities. An esophagogram is an x-ray study in which a radiologist takes images of a person swallowing a liquid. The Zenker’s Diverticulum is seen on this study.
Treatment
The treatment for a Zenker’s Diverticulum is cutting the cricopharyngeus muscle, known as a cricopharyngeal myotomy. When this muscle is cut the throat relaxes, making swallowing easier. There are two major ways to this. A minimally invasive approach is to cut the muscle through the mouth. This procedure takes approximately 30 minutes to perform. A carbon dioxide laser or a stapler is used to perform the surgery known as Zenker’s Diverticulectomy.
Jamin Brahmbhatt, MD, is a board-certified urologist and Chief of Surgery at Orlando Health South Lake Hospital.
Your urethra is a tube through which urine from your bladder flows through to leave the body when you urinate. A urethral diverticulum (UD) is a pocket or pouch that forms along the length of your urethra. This pocket, because of where it’s positioned, gets continuously filled with urine when you urinate, and this sometimes leads to pain, problems urinating, frequent infections, and urinary incontinence.
Although rare, urethral diverticulum can also lead to the formation of urethral calculus, a hard stone formed in the urethra as a result of the build-up of stagnant urine and salt deposits in the diverticulum.
Notwithstanding the fact that the number of diagnoses for it is rising, urethral diverticulum is generally not a common condition. The medical community speculates that its increasing prevalence is simply because of the existence of more sophisticated imaging techniques leading to more diagnoses than in the past. Urethral diverticulum is generally more common in women than men.
Symptoms
Symptoms of urethral diverticulum vary, and their presence and severity are usually unrelated to the size if the pouch/sac. Indeed, you may have a urethral diverticulum and be asymptomatic (not experience any symptoms).
Some of the common symptoms of this conditions are:
- Pain while urinating (dysuria)
- Blood in urine (hematuria)
- Leaking or dribbling after urinating
- Recurrent cystitis
- Frequent unitary tract infections (UTIs)
- Painful sexual intercourse
- Tender area or mass on the vaginal wall
- Bladder infections
- Pelvic pain
You may only experience some but not all of these symptoms. In addition, they may not be constant—they may disappear for long periods of time only to return later on.
Causes
You may be born with a urethral diverticulum or you may acquire one. Congenital urethral diverticulum (present from birth) usually stems from Gartner duct cysts and Müllerian duct cysts. The cause of acquired urethral diverticulum isn’t always known but it has been linked to obstruction of the urethral glands and multiple bladder infections that are thought to weaken the walls of the urethra. Trauma during a vaginal birth has also been identified as a contributor to the formation of urethral diverticulum.
Diagnosis
The symptoms of urethral diverticulum are not specific—it shares the symptoms of many other bladder or urethra related conditions. Some people are misdiagnosed and treated for other conditions like cystitis and vulvodynia for many years. It’s also sometimes diagnosed completely by accident, like when imaging tests for entirely different reasons are carried out.
The most reliable ways urethral diverticulum can be diagnosed by your doctor are:
- Physical examination: In women, the walls of the vagina can be examined and felt for tender masses or areas. Also, your doctor may try to express pus or urine from the urethral diverticulum space.
- Ultrasonography: This method will involve using ultra (high frequency) sound waves to obtain pictures of your urethra and surrounding structures.
- Cystoscopy: A cystoscopy is an in-office procedure in which the doctor places a camera connected to a long tube into your urethra and bladde. This procedure can help in the diagnosis of a urethral diverticulum.
- Magnetic resonance imaging (MRI):MRI uses a large magnet and radio waves and a magnetic field to produce clear images of the body. In this case, it will be used to get detailed images of your pelvic area and vagina to detect any abnormalities. Currently, this is accepted as the best test to diagnose urethral diverticulum.
- Voiding cystourethrogram (VCUG): This involves an X-ray of your bladder and urinary tract taken while you are urinating.
Treatment
Surgical excision is the main way to treat symptomatic urethral diverticulum.
Because of its highly technical nature, if you choose to have surgery, it will have to be performed by a specialist called a urogynecologist.
The surgical options you have include:
- A complete removal or the pocket/sac. This is the most likely route your doctor will recommend.
- Cutting into the neck of the pocket/sac and draining its contents completely.
- Spence Procedure, which involves making an opening of the urethral diverticulum into the vagina. That is, an opening will be made for the contents of the sac/pocket to be able to flow out through the vagina.
Any infection you may have must first be resolved before surgery can be performed.
The surgical option chosen depends on the size and location of the urethral diverticulum, as well as other factors identified by your doctor. During your surgery, your surgeon may also be to fix any incontinence issues you may have been experiencing. After surgery, you’ll likely be given some antibiotics for at least 24 hours to prevent infections. You may also be fitted with a catheter that’ll remain in place for some weeks for better healing. You’ll be instructed to show up for follow-up tests in subsequent weeks to check the success of the surgery, the status of your healing, and to remove the catheter.
There are some side effects you risk from having any of these surgical procedures, such as serious bleeding, recurrence of the urethral diverticulum, infection, urethrovaginal fistula, and urethral scarring. You should discuss all of these with your doctor before consenting to the surgery.
Alternatively, you may want to wait to see if your symptoms get worse or the urethral diverticulum gets bigger before considering surgery. It is also possible that you don’t want to undergo surgery at all. In that case, your doctor will help devise a management plan with you. However, you should know that, as it stands, not much is known about leaving urethral diverticulum untreated—there’s no way to know if the pockets will get bigger or if your symptoms will worsen.
You should also know that, although it’s very rare, there have been cases of people with urethral diverticulum developing carcinoma (a type of cancer).
A Word From Verywell
If you’ve been diagnosed with urethral diverticulum, it is important that you discuss your options extensively with your doctor. You do not have to go through with having surgery if you don’t want to and your doctor agrees that it is not medically necessary.
If you have opted to have surgery, it is natural for you to feel anxious or worried about the procedure and the possible outcomes. Your doctor should give you the details of what you should expect before, during, and after the surgery. It is advisable that you have positive yet realistic expectations of your surgical outcomes, and prepare for the possibility of the urethral diverticulum recurring.
You should consider speaking to your family and loved ones about any anxiety or fears you may have about the surgery. You could also consider seeing a counselor/therapist for a more professional approach—we find that some hospitals provide pre-surgery counseling sessions.
Table of Contents
Image: “Stadien des Zenkerdivertikels von Brombart 1 bis 4” by Hellerhoff. License: CC BY-SA 3.0
Definition and Pathogenesis of Diverticula
True and false diverticula
Diverticula are wall protrusions in hollow organs. A distinction must be made between ‘true’ and ‘false’ diverticula. Medical students should learn the definitions and differences, as they usually appear on medical student exams, particularly Zenker’s diverticulum.
True diverticula
In the case of a true diverticulum, all wall layers are affected, even the muscularis. The protrusion often occurs due to tension from outside, such as scarring or inflammatory changes (with tuberculosis or lymphadenitis, for example).
False diverticula
In the case of a false diverticulum (or pseudo-diverticulum), only mucosa and submucosa evert to the outside through a weak spot in the muscle layer. The reason for this is increased intraluminal pressure.
With respect to the esophagus, diverticula can be classified on the basis of location, as well as whether they are true or false.
Traction diverticula
Traction diverticula are true diverticula and are usually found on the level of the tracheal bifurcation. Therefore, they also are referred to as bifurcation diverticula or parabronchial diverticula.
Pulsion diverticula
Pulsion diverticula are false diverticula. Predilection sites include the following points of the esophagus that have weak muscle:
- Laimer triangle (longitudinal muscle-free zone on the upper esophagus)
- Killian triangle (muscle-weak area between the pars obliqua and the pars fundiformis of the cricopharyngeal muscle of the dorsal hypopharynx). Strictly speaking, this is really a diverticulum of the hypopharynx, although it is usually dealt within the context of the esophagus. Diverticula in the area of the Killian triangle are also known as Zenker’s diverticula.
- Above the diaphragm: called an epiphrenic diverticulum
Epidemiology of Zenker’s Diverticulum
Zenker’s diverticulum is the most common type. It represents 70% of all cases of diverticula, followed by traction diverticula (20%) and epiphrenic diverticula (10%). Zenker’s diverticulum affects mostly older men.
Symptoms of Esophageal Diverticula
Dysphagia and regurgitation
Large diverticula are accompanied by symptoms. Patients complain of dysphagia, retrosternal pain, feelings of pressure, and nightly regurgitation of undigested food residue. The latter is associated with risks of aspiration and pneumonia. The deposition of food residue in the bulges may lead to halitosis. Some patients describe a ‘gurgling’ sound when they drink.
Diverticula rarely become inflamed, bleed, perforate, or form fistulas.
Image: Barium esophagram revealing traction esophageal diverticulum with communication into the right upper lobe segmental bronchi. By Openi, License: CC BY 2.0
Diagnosis of Esophageal Diverticula
Image: Normal barium swallow fluoroscopic image, showing the ingested barium sulfate being induced down the oesophagus by peristalsis. By Bernd Brägelmann, License: CC BY 3.0
Esophageal bolus swallow test is the method of choice
The diagnostic method of choice is an esophageal bolus swallow test. X-ray images often clearly show the accumulation of contrast agents in protuberances, allowing precise differentiation of diverticula according to their location. Traction diverticula usually feature ‘ear-like’ outgrowths, whereas pulsion diverticula are mainly sack-shaped.
Due to the possible presence of a perforation, in the United States, it is recommended that healthcare professionals use a water-soluble contrast medium, as barium poses the risk of mediastinitis or peritonitis upon exit from the esophagus.
Endoscopy
In order to exclude other possible causes of symptoms, endoscopy always should be performed as well. However, care must be taken because the mucous membranes near diverticula are particularly prone to perforation.
Differential Diagnoses
In terms of differential diagnoses, healthcare practitioners should consider esophageal carcinoma.
Therapy of Zenker’s Diverticulum
Surgical measures for Zenker’s diverticula
Diverticula can be treated surgically. However, surgery is usually indicated only for Zenker’s diverticula—rarely for larger and symptomatic epiphrenic diverticula.
Affiliations
- 1 Department of Radiodiagnosis, Pushpagiri Institute of Medical Sciences, Tiruvalla, Kerala, India.
- 2 Department of General Medicine, Pushpagiri Institute of Medical Sciences, Tiruvalla, Kerala, India.
- PMID: 28607626
- PMCID: PMC5448610
- DOI: 10.12659/PJR.899248
Free PMC article
Authors
Affiliations
- 1 Department of Radiodiagnosis, Pushpagiri Institute of Medical Sciences, Tiruvalla, Kerala, India.
- 2 Department of General Medicine, Pushpagiri Institute of Medical Sciences, Tiruvalla, Kerala, India.
- PMID: 28607626
- PMCID: PMC5448610
- DOI: 10.12659/PJR.899248
Abstract
Background: Mid-esophageal region is an uncommon location of esophageal diverticula, a condition usually diagnosed in elderly individuals.
Case report: We report a case of an elderly male with incidental finding of mediastinal lesion, which was initially thought to be an aortic aneurysm. Further evaluation demonstrated a mid-esophageal diverticulum at the level of the carina. We present patient’s medical history and imaging, followed by a discussion on symptoms and management.
Conclusions: Knowledge of benign conditions that might mimic a mediastinal vascular pathology is important for therapeutic and prognostic reasons, as they are often managed conservatively.
Keywords: Deglutition Disorders; Diverticulum, Esophageal; Esophageal Motility Disorders; Esophagectomy; Mediastinum.
Esophageal Diverticulum – Definition, Causes, Symptoms, Risk Factors, Screening Tests, Diagnosis, Treatments, Medications, Home Remedies, Alternative Therapies, Clinical Trials, Medical Research Studies, Prevention, Coping, Lifestyle Changes, Self-Help
- Post author
Esophageal Diverticulum – Definition, Causes, Symptoms, Diagnosis, Treatment, Home Remedies, and Prevention
New York (USA), December 05, 2017
Definition, Diagnosis, and Pathophysiology of Esophageal Diverticulum
Causes, Evaluation, and Medical Assessment of Esophageal Diverticulum
The Most Common Signs and Symptoms of Esophageal Diverticulum
Complications, Prevalence, Prognosis, and Risk Factors for Esophageal Diverticulum
Screening Laboratory Tests and Diagnostic Procedures for Esophageal Diverticulum
Treatment Options, Medications, and Management of Esophageal Diverticulum
Clinical Trials and Medical Research Studies on Esophageal Diverticulum
Alternative Therapies, Home Remedies, and Natural Cures for Esophageal Diverticulum
Prevention Tips and Coping Strategies for Esophageal Diverticulum
Frequently Asked Questions, Lifestyle Changes, and Self-Help Tips for Esophageal Diverticulum
Laparoscopic Esophageal Diverticulum Resection with Long Esophageal Myotomy
2009-08-11 Janos Taller
Dr. Janos Taller of San Diego Minimally Invasive Surgery () performs an advanced laparoscopic resection of an epiphrenic diverticulum .
Zenker’s Diverticulum Surgery – Endoscopic Staple Diverticulostomy
2012-04-27 Fauquier ENT
– This video shows how endoscopic staple diverticulostomy (ESD) is performed to correct a Zenker’s Diverticulum. For more .
ESOPHAGEAL DIVERTICULUM
2013-05-21 purushottam vashistha
a 80 yrs old male presented with dysphagia without any alarming symptoms found to have a large esophageal diverticulum at lower end with tight LES .
Esophageal diverticula
This topic discuss the different types of esophageal diverticula.
Esophageal Diverticulum Resection
2016-09-25 Ziad Awad
Thoracoscopic Resection of Mid Esophageal Diverticulum.
Thoracoscopic resection of mid-esophageal diverticulum
2017-07-10 Society of American Gastrointestinal and Endoscopic Surgeons (SAGES)
Presented by Andrew J Fritze, MD at the SS22: Friday Exhibit Hall Video Presentations Session 3 held during the 2017 SAGES Annual Meeting in Houston, .
Dr Pradeep Jain -Laparoscopic Resection Epiphrenic Esophageal Diverticulum
2014-04-14 Pradeep Jain
Dr Pradeep Jain is currently appointed the Chief of Department GI, GI Onco, Bariatric & MinimalAccessSurgery, at Action Cancer Hospital & Sri Balaji Action .
Laparoscopic resection of esophageal diverticulum
2016-07-03 Trakia Park Surgery / Хирургия Тракия Парк
This vieo presents laparoscopic transhiatal resection of epiphrenic esophageal diverticulum. Hiatoplasty and Toupet fundoplication were additionally performed.
Targeted POEM to treat small mid-esophageal diverticulum
2017-07-07 Society of American Gastrointestinal and Endoscopic Surgeons (SAGES)
Presented by Toshitaka Hoppo, MD, PhD at the SS16: Friday Exhibit Hall Video Presentations Session 1 held during the 2017 SAGES Annual Meeting in .
Laparoscopic resection of subphrenic esophageal diverticulum complicated by perforation
Surgery team: Prof. Starkov Yu.G., MD., PhD Shishin K.V., MD., PhD Vyborniy M.I. Video Editing: Vyborniy M.I..
Diverticula, diverticulosis, & diverticulitis – causes, symptoms & pathology
What are diverticula? Diverticula are outpouchings that most commonly happen in the sigmoid colon of the large intestine. The presence of a diverticulum is .
Laparoscopic Approach to a Subphrenic Esophageal Diverticulum
View the full article here:
Epiphrenic esophageal diverticulum short version HD
Laparoscopic approach and surgical considerations in resection of a large epi-phrenic esophageal diverticulum.
Trans-Oral Laser for the Treatment of Zenker’s Diverticulum | Dr. Babak Larian in Los Angeles
Learn about trans-oral laser for the treatment of Zenker’s Diverticulum from Los Angeles ENT, Dr. Babak Larian – Dr. Babak Larian, .
Surgery: Esophagus (Zenker Diverticula)1
2014-06-07 dr abhi b
I am a medical student studing in Grant Medical College, Mumbai, Maharashtra university of Health Science, India. Have a keen desire to explain the different .
Mid-esophageal diverticulum
2014-06-20 GI Motility
ESOPHAGEAL DIVERTICULUM CHRISTOS KARALIS.wmv
2010-01-19 Christos Karalis
ОџО№ПѓОїП†О±ОіО№ОєПЊ ОµОєОєПЊО»ПЂП‰ОјО± ПѓОµ О±ПѓОёОµОЅО® ОјОµ ОїО№ПѓОїП†О±ОіО№ОєО® ОґП…ПѓОєО№ОЅО·ПѓОЇО±. Esophageal diverticulum in a patient with esophageal dysmotility diorder.
oesophageal diverticula
2016-11-07 creative medicine
I created this video with the YouTube Video Editor ()
esophageal diverticula diet
2016-03-24 Римма Захарова
Laparoscopic Resection of Epiphrenic Diverticulum
2014-09-15 Society of American Gastrointestinal and Endoscopic Surgeons (SAGES)